Trigeminal Neuralgia
POSTED: 2/13/2023

Trigeminal Neuralgia
Monday, February 13, 2023
What is Neuralgia?
To better understand trigeminal neuralgia, it is important to distinguish two entities. Neuralgia and neuropathy. Neuralgia refers to paroxysms of brief lancinating pain in the distribution of a peripheral nerve. Examples include trigeminal neuralgia, occipital neuralgia, and glossopharyngeal neuralgia.
In contrast, neuropathy is a dysfunction of said peripheral nerve that may or may not result in pain and false sense of swelling. While the pain of neuralgia is often described as sharp, stabbing, and shock-like, pain from neuropathy is more often a burning or prickling sensation.
Trigeminal neuralgia definition:
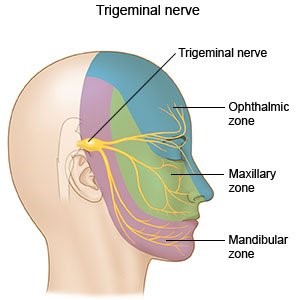
To better understand this facial pain syndrome, a good understanding of the location and function of the trigeminal nerve is important. The trigeminal nerve provides sensation to the face from the mandible to the vertex of the head anteriorly through three divisions referred as ophthalmic (V1), maxillary (V2), and mandibular (V3). The latter also provides motor fibers to some of the muscles of mastication. A picture depiction of the trigeminal nerve is found below. While considered a peripheral nerve, the base of the trigeminal nerve is house in the brainstem.
Given the complexity of trigeminal neuralgia and advances in medical technology, its definition evolved over the years to the current one set forth by the International Classification of headache Disorders, third Edition (ICHD-3). Trigeminal neuralgia is defined as recurrent paroxysms of unilateral facial pain confined to one or more divisions of the trigeminal nerve without spread beyond the nerve distribution. The pain is severe in intensity, lasting a fraction of a second to no more than two minutes, and described as shock like, shooting, stabbing, or sharp. The pain must be precipitated by innocuous stimuli and reproducible.
Trigeminal neuralgia classification:
Trigeminal neuralgia can be classified by symptomatology or by etiology. The two are often used hand in hand in the clinical setting. If the pain of trigeminal neuralgia is the result of a compression by a neighboring artery, this is referred to as classical trigeminal neuralgia. If the pain of trigeminal neuralgia is the result of a separate intracranial process such as a tumor, multiple sclerosis (inflammatory disease of the brain and spine), stroke, or vascular malformation, this is termed secondary trigeminal neuralgia. Lastly, if the pain of trigeminal neuralgia is associated with no cause evident by MRI or electrophysiologic tests, this is referred to as idiopathic trigeminal neuralgia.
Another classification scheme of trigeminal neuralgia employs the nature of symptoms and their duration. The vast majority of patients with trigeminal neuralgia have recurrent paroxysms of pain as defined above with complete pain freedom between attacks. This is referred to as classical trigeminal neuralgia or Type I. A subset of patients however has continuous or near continuous background pain in the same distribution in between classical attacks and this is termed classical trigeminal neuralgia with concomitant continuous pain or Type II. Irrespective of the classification used, patients with trigeminal neuralgia do no have sensory loss in the area affected. As such, numbness should prompt evaluation for a painful trigeminal neuropathy.
Epidemiology and symptomatology:
Trigeminal neuralgia is a rare disorder that affects women more so than men with a ratio of up to 1.7:1. Its prevalence is not thought to exceed 0.3% of the general population. While this disorder can occur at any age, the average age of onset is greater than fifty years. Secondary and idiopathic trigeminal neuralgia tends to affects younger patients compared to neurovascular compression. In most instances, this is a sporadic occurrence, however, a family history is reported in up to 11% of patients with trigeminal neuralgia.
While each paroxysm of pain is brief, patients often experience a series of attacks or a cluster that can last up to an hour. This is usually followed by a burn out period where no pain can be elicited or the intensity is reduced. Approximately 99% of patients with trigeminal neuralgia report their pain is triggered by activating maneuvers such as talking, chewing, brushing their teeth, eating, shaving, applying make-up, touching the face, washing the face, and cold wind contacting the face. As such, and given the severity of the pain, this disorder can be disabling. There is no particular pattern for these attacks and periods of remission up to years are possible.
The right trigeminal nerve tends to be affected more than the left trigeminal nerve, and in most instances, V2 and or V3 are involved with rare cases of V1 involvement. Bilateral trigeminal neuralgia is exceedingly rare and should always prompt evaluation for secondary cause.
Diagnosis and Treatment:
When a patient presents with recurrent and brief attacks of facial pain as defined above without significant facial numbness, a diagnosis of trigeminal neuralgia can be made. However, use of MRI imaging is key as it aids in the classification of the trigeminal neuralgia and subsequently treatment.
Regardless of cause or type, all forms of trigeminal neuralgia can be treated medically initially in an attempt to prevent or delay surgical intervention. Pharmacological agents are classified as preventatives or rescue. The former is taken on a regular basis to reduce attack frequency and severity, while the latter is used for acute exacerbation without remission. The mainstay preventatives are two anti-seizure medications, Carbamazepine (Tegretol) or Oxcarbazepine (Trileptal), that reduce excitability of the nerve by blocking sodium channels. If these fail or are not tolerated, use of second line agents is often done and include other anti-seizure medications such as Valproate (Depakote), Lamotrigine (Lamictal), Gabapentin (Neurontin), Topiramate (Topamax), and Baclofen. If oral medications prove helpless and surgery is not desired, use of Botox injections can alleviate pain at times and is currently under further investigation as a treatment for trigeminal neuralgia. In cases of exacerbations, intravenous Phenytoin (Dilantin), another anti-seizure medication, or Lidocaine can be infused to alleviate pain as rescues.
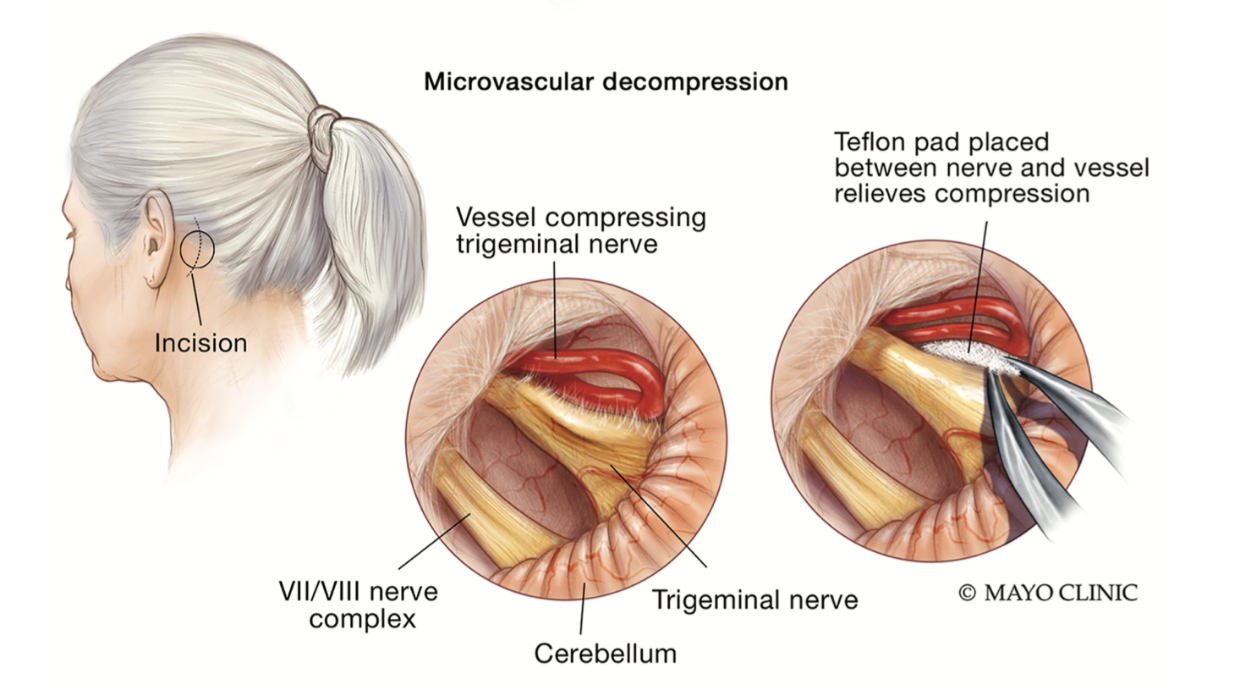
A specific MRI protocol is used to acquire close up images of the trigeminal nerve exiting the brainstem and its relation to neighboring arteries. If the adjacent artery is not only contacting the trigeminal nerve, but also resulting in loss of its fibers and or its displacement, then surgical decompression of the nerve can be curative. This procedure is referred to as microvascular decompression and is performed by a neurosurgeon as a first line surgical treatment option.
If a patient fails oral medications and is not found a candidate for microvascular decompression by imaging, other surgical interventions remain possible. Neuroablation is a treatment modality that targets the nerve directly and includes balloon compression, glycerol injection, and radiofrequency thermocoagulation. In other words, using various means, these techniques aim at injuring the trigeminal nerve enough to reduce the severity of the pain.
If you or a loved believe to be suffering from trigeminal neuralgia, please contact the neurology clinic at 337-374-7242 for an appointment.
Oliver Achi, MD
Medical Director of Neurology Services
Iberia Medical Center